Pelvis/Hip Case 12 Management
VS Pelvic fractures are typically associated with high-speed mechanisms and other critical injuries, so follow principles of ATLS first and foremost. Definitive hemorrhage control can be achieved by embolization in Interventional Radiology or by the surgeon in the operating room. These decisions depend on institutional resources and whether the patient has other surgical indications.
The specific definitive management of pelvic fractures requires orthopedic consultation Since pelvic volume is increased in VS injuries, hemorrhage risk is higher. Pelvic binders or bed sheets can be used to temporarily provide some rotational stability to the pelvis. Pelvic binders also decrease pelvic volume and can temporarily control venous bleeding by tamponade effect but are unlikely to control arterial bleeding. Pelvic binders stabilize the pelvis rotationally but not vertically, so VS injuries will still be vertically unstable despite placement of a binder. Make sure to center the binder over the trochanters, not the iliac crests.
Avoid Foley catheter placement until urethral injury has been ruled out if there is:
- Blood at the urethral meatus
- Inability to void
- Gross hematuria
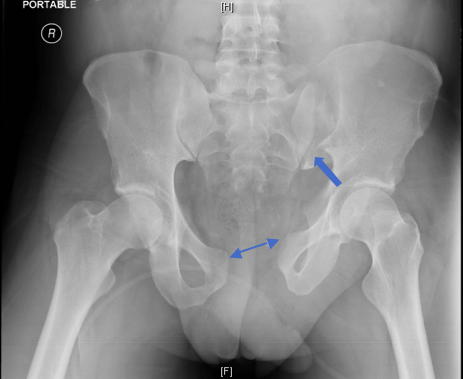
- Straddle fractures, vertical shear fractures, or disruption of the anterior and posterior pelvic ring