Posterior Shoulder Dislocation
These are TRICKY. The classic boards presentation is shoulder pain after a seizure or lightning strike, but these can occur with simple falls too. These dislocations tend to be more subtle and less dramatically displaced than most anterior dislocations and are easy to miss, so the provider must maintain a high index of suspicion when the scenario is suspicious (i.e. seizure). The patient often does not have an obvious deformity on exam.
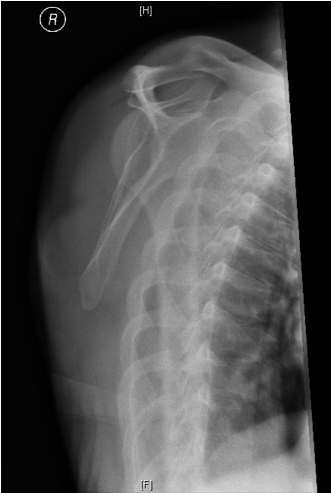
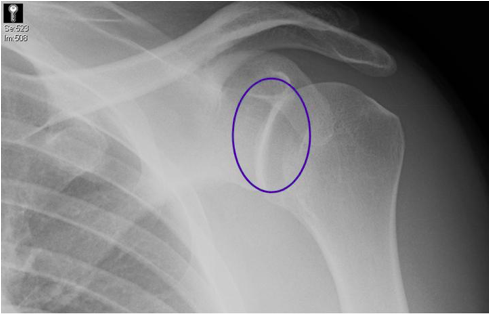
This is an example of a difficult to appreciate posterior dislocation. The humeral head appears to be in the Y. The clinical scenario, however, of pain and loss of range of motion after a seizure was highly suspicious for posterior dislocation, so further views are needed.
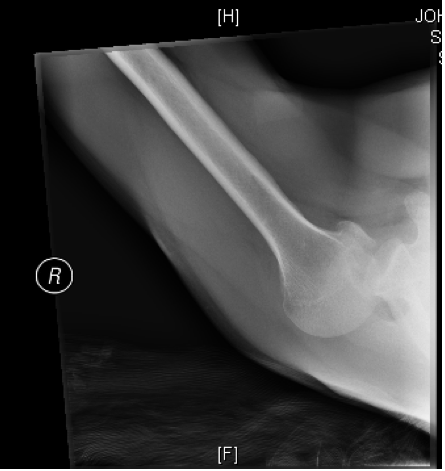
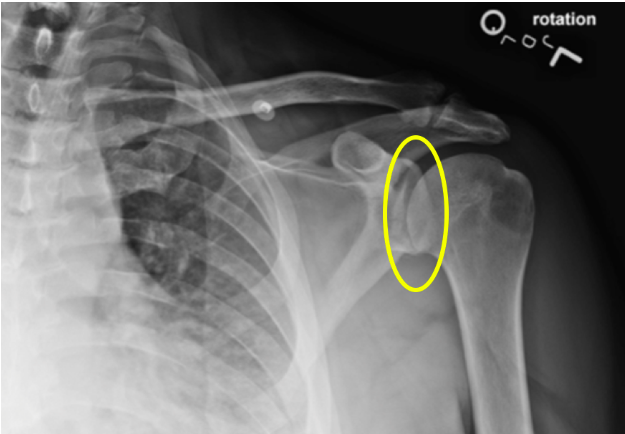
Axillary View of the same patient (below) done after the equivocal Y view, confirming posterior dislocation. Note how the humeral head is not sitting in the glenoid (think of it like a golf ball falling off the tee). It has displaced toward the side of the acromion, making this a posterior dislocation.
Other clues on XRs to posterior dislocations:
- “Cystic” or “hollowed out” appearance of the humeral head
- “Trough line sign” signifying impaction fracture of the humeral head against the glenoid upon dislocating
- Possible absence of the normal elliptically-shaped overlap of the humeral head with the glenoid on the AP internal rotation view
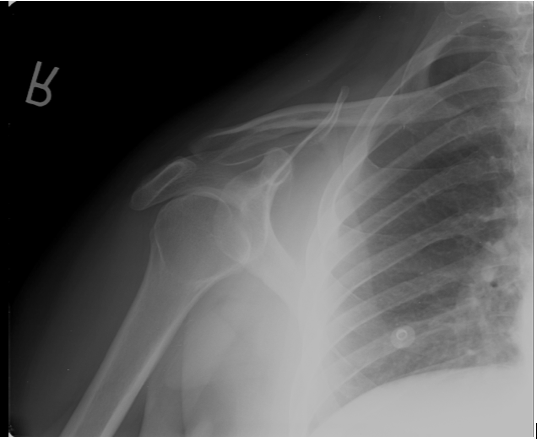
Below is an example of cystic humeral head. The humeral head is internally rotated in posterior dislocation so that the greater tuberosity is anterior. The tuberosity then attenuates the beam leaving the humeral head appearing “cystic” or “hollowed out”.
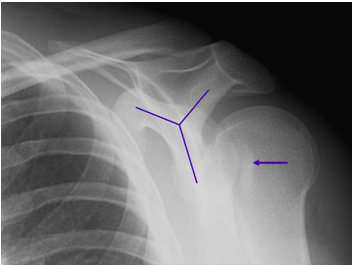
Below is an example of an impaction fracture. The arrow indicates fracture from the humeral head impacting against the rim of the glenoid after dislocating posteriorly. This is known as the “trough line sign” because it resembles the trough lines on a weather map. The x ray also shows that the humeral head is posterior to the Y.
Below is an example of abnormal glenohumeral articulation in posterior dislocation. A normal glenohumeral articulation has elliptical overlap of the glenoid and humeral head on the AP internal rotation view. That overlap is lost in this posterior dislocation.
Versus a normal elliptical overlap as below
Things to keep in mind:
- Get a TRUE Y-VIEW if you are suspicious for dislocation
- If the diagnosis of posterior dislocation is still unclear, get an AXILLARY VIEW. This will likely require analgesia since positioning for this view is painful in the setting of fracture or dislocation.