Hand Case 3 ED Management
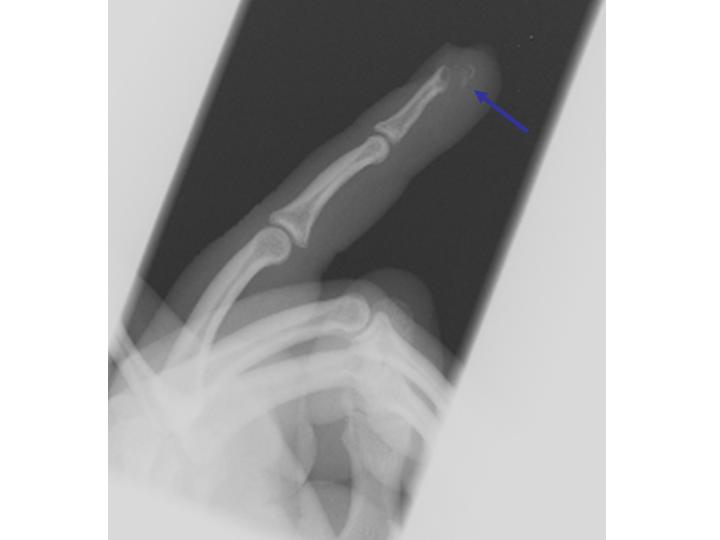
Comminuted open distal tuft fracture
ED Management
Treatment is mainly focused on the soft tissue injury. Immobilization is typically unnecessary, although a short volar or hairpin splint can be used to protect the finger tip for 2-3 days to prevent further trauma. Splinting, if elected, should not involve the PIP joint. Patients will often require analgesia.
Most tuft fractures are comminuted and involve the nail bed. Management of these injuries depends on the condition of the nail:
- If the nail plate is intact, leave it in place. Drainage of the subungual hematoma can be carried out by trephination of the nail.
- Damage or loss of the nail plate requires nail removal, nail bed repair with 6-0 chromic suture, and protection.
Irrigation, debridement, and IV antibiotics are indicated for open tuft fractures. The patient may be discharged home with prompt referral to a hand surgeon.
Surgery is indicated if the dorsal surface of the phalanx that supports the nail matrix has significant step-off, especially with concomitant nail plate avulsion. When this occurs, a hand specialist should reduce the fracture to an even surface and pin it to support the surgical repair of the nail matrix.
Although usually benign, tuft fractures can have significant morbidity. Up to 70% had bothersome symptoms, including numbness, hyperesthesia, and cold sensitivity, at 6 months. Therefore, non-urgent referral to a hand specialist is recommended.